Abstract
Drug addiction remains a critical public health challenge, particularly in developing countries like Kenya, where access to effective rehabilitation services is limited. Understanding the factors that influence recovery time is essential for improving treatment outcomes and informing evidence-based interventions. This study aimed to model recovery time among drug-addicted individuals using survival analysis techniques and to identify key determinants influencing the rate of recovery. This study focuses on applying the Cox PH model to estimate recovery hazard rates and identify significant predictors among individuals receiving treatment. A retrospective cohort design was employed using secondary data obtained from a rehabilitation facility in Kericho County, Kenya, covering the period 2021 to 2025. The key findings indicate that education level (HR 1.18, p=0.049) and Substance Type (Multiple Drugs vs. Alcohol, HR 0.67, p=0.027) are significant predictors of recovery from drug addiction. Specifically, higher education levels are associated with a higher hazard of recovery, likely due to enhanced health literacy. At the same time, individuals using multiple substances face a lower hazard of recovery compared to those using alcohol only, reflecting the clinical complexity of polysubstance use. The Cox PH model satisfied the proportional hazards assumption (Global p=0.24), confirming its adequacy for the data. These results highlight the importance of socio-demographic and substance-related factors in recovery from drug addiction. In practice, treatment facilities/rehabilitation centers should integrate health literacy enhancement programs specifically for individuals with lower education levels to improve treatment adherence and accelerate recovery. Besides, more intensive and prolonged interventions, such as enhanced counseling, specialized therapy, and closer monitoring, are recommended for polysubstance users to address their greater clinical needs. For policy, the study’s results underscore the need to develop substance-specific treatment guidelines, increase resource allocation for polysubstance addiction programs, and implement standardized drug-user data recording systems in rehabilitation facilities across Kenya. These strategies will improve recovery outcomes, optimize service delivery, and strengthen national efforts for reducing the burden of drug addiction.
Keywords
Cox PH Model, Survival Analysis, Drug Addiction, Recovery Rates, Hazard Rates, Proportional Hazards
1. Introduction
Drug addiction is a critical global and national public health challenge. According to the United Nations Office on Drugs and Crime (UNODC)
, about 296 million people aged 15–64 used at least one drug in 2021. In Kenya, the 2022 National Survey on the Status of Drugs and Substance Use shows that approximately 4.7 million individuals aged 15–65 years use at least one drug or substance
. This burden is high primarily among young people aged 25–35 years, a population with transition, vulnerability, and elevated risk factors, where 42.4% of alcohol users and 47.4% of cannabis users meet the threshold for addiction
.
Multifaceted interventions are necessary to achieve recovery from drug addiction. Most studies on drug addiction in Kenya have been cross-sectional and descriptive, failing to capture the longitudinal nature of recovery or the influence of time-varying covariates. This study sought to fill this gap by applying the Cox PH model, a survival analysis statistical method for evaluating the time to an event (in this case, recovery) while accounting for censored data and including explanatory variables.
Kasisi
used this model in Kenya to identify significant predictors, such as age and gender, but did not evaluate other potentially significant predictors, such as education level. Recent reports by NACADA identified Kericho County as a hot spot for drug use and trafficking
. These local dynamics further justify the need for data-driven models to understand and improve recovery outcomes at the community level. This study contributes to the growing literature on recovery from drug addiction by offering a predictive model of treatment success. By modeling time-to-recovery using the Cox PH model, this study provides practical insights for guiding clinical practices, policy formulation, and targeted interventions for people struggling with drug addiction in Kenya.
Various researchers have used different models or approaches to evaluate the recovery from drug addiction. In high-income settings, Kim and Suh
| [8] | S. Kim and H. S. Suh, “A population-based study on the risk of prescription opioid abuse in patients with chronic opioid use and cost-effectiveness of prescription drug monitoring program using a patient simulation model in South Korea,” International Journal of Drug Policy, vol. 112, p. 103953, Feb. 2023,
https://doi.org/10.1016/j.drugpo.2023.103953 |
[8]
used the Cox PH model to identify risk factors for opioid abuse in South Korea. The study highlights the effectiveness of the Cox PH model in predicting hazards for time-to-event data. However, it only focuses on opioid abuse rather than recovery, limiting direct applicability to recovery time. It also excludes substances such as alcohol and tobacco, which are central to this study in Kericho County, Kenya. Therefore, although their study underscores the Cox PH model’s versatility, it highlights the gap in recovery-focused studies for non-opioid substances in developing countries like Kenya.
Lu et al.
| [12] | W. Lu, T. Lopez-Castro, and T. Vu, “Population-based examination of substance use disorders and treatment use among US young adults in the National Survey on Drug Use and Health, 2011–2019,” Drug and Alcohol Dependence Reports, vol. 8, p. 100181, Sep. 2023,
https://doi.org/10.1016/j.dadr.2023.100181 |
[12]
used logistic regression to examine substance use disorder (SUD) prevalence and treatment among US young adults (aged 18–25). The study’s results show a significant overall increase in SUD prevalence, highlighting the socio-demographic influences on treatment, but underscore the gap in survival analysis-based recovery studies. Although it focuses on treatment engagement and covariates like gender and education, as well as the substance scope, including alcohol and illicit drugs, it lacks survival analysis, specifically the use of an appropriate model like the Cox PH model for modeling recovery from SUD.
Das et al.
| [4] | D. Das, H. Saikia, D. Bora, D. Bhattacharjee, and J. Das, “A survival analysis approach for identifying the risk factors in time to recovery of COVID-19 patients using Cox proportional hazard model,” Decision Analytics Journal, vol. 5, p. 100137, Dec. 2022, https://doi.org/10.1016/j.dajour.2022.100137 |
[4]
used the Cox PH model to analyze the time to recovery among COVID-19 patients in India. The researchers identified significant risk factors affecting recovery time, including pre-disease status, location, and food habits. Using the Cox PH model emphasizes its usability and interpretability for analyzing time to recovery. Therefore, it allows using the model of recovery from different conditions or diseases, including recovery from drug addiction, the focus of this study.
In their qualitative study using lifeline interviews, Martinelli et al.
| [13] | T. F. Martinelli, D. Roeg, L. Bellaert, van, and G. E. Nagelhout, “Understanding the Process of Drug Addiction Recovery Through First-Hand Experiences: A Qualitative Study in the Netherlands Using Lifeline Interviews,” Qualitative Health Research, vol. 33, no. 10, pp. 857–870, Jun. 2023,
https://doi.org/10.1177/10497323231174161 |
[13]
used data-driven thematic analysis to examine the drug addiction recovery process. The researchers noted four themes that the participants identified as part of the recovery process: addiction is interlinked with everything, drug addiction recovery is reconsidering identity, it is a long-term process, and universal life processes constitute the recovery process. This study is insightful on how persons with drug addiction experience recovery over time, forming the basis for developing more specific models to examine the recovery process with particular considerations of demographic, economic, and other factors.
Iswardani et al.
| [6] | T. Iswardani, Z. L. Dewi, W. W. Mansoer, and I. Irwanto, “Meaning-Making among Drug Addicts during Drug Addiction Recovery from the Perspective of the Meaning-Making Model,” Psych, vol. 4, no. 3, pp. 589–604, Sep. 2022,
https://doi.org/10.3390/psych4030045 |
[6]
used a conceptual framework grounded in the Meaning-Making Model to understand changes in recovery from drug addiction. This model provides a theoretical framework for examining the complex recovery process, and the researchers created a complex illustration of the role of meaning-making in the recovery process by integrating components such as coping mechanisms and adverse childhood experiences (ACE) into their analysis. Besides, the study aligns with more comprehensive models of addiction recovery, such as the bio-psycho-social-spiritual (BPSS) model and the Developmental Model of Recovery (DMR), which emphasize the importance of addressing social, psychological, biological, and spiritual facets to enhance long-term recovery.
Ling et al.
studied the recovery from opioid use disorder (OUD) after following the administration of the long-acting buprenorphine subcutaneous injection (BUP-XR) as treatment. Within the conceptual framework of the RECOVER observational study, the study evaluated the relationship between the length of BUP-XR medication. It sustained opioid abstinence, considering the potential variables using multiple regression models. The study also looked at changes in depression, pain thresholds, work status, health-related quality of life, and withdrawal symptoms as factors contributing to recovery advancement. The study provides insights into the complex dynamics of OUD recovery, highlighting the long-term effects of treatment on patient-centered outcomes.
Moeeni et al.
| [14] | M. Moeeni, E. M. Razaghi, K. Ponnet, F. Torabi, S. A. Shafiee, and T. Pashaei, “Predictors of time to relapse in amphetamine-type substance users in the matrix treatment program in Iran: a Cox proportional hazard model application,” BMC Psychiatry, vol. 16, no. 1, Jul. 2016,
https://doi.org/10.1186/s12888-016-0973-8 |
[14]
’s study determined the predictors affecting the risk of relapse among amphetamine-type substance (ATS) users in Iran. The study primarily used participants’ age, marital status, sex, employment status, and high school graduation status to assess the time to relapse using the Cox PH model.
In the African context, there is still limited evidence on recovery from drug addiction. Most studies are descriptive or cross-sectional rather than employing survival analysis. A systematic review of substance use and substance use disorders in Kenya by Jaguga et al.
highlighted the high burden of substance use and the scarcity of robust intervention studies, noting that available treatment programs often lack systematic evaluation of outcomes such as time to recovery. This review also particularly noted that most intervention studies in the region have focused on alcohol only, excluding other prevalent substances like cigarettes and cannabis, suggesting the need for more research on substance use in Kenya.
In addition, the systematic review by Biribawa et al.
on treatment outcomes for substance use disorders across the African continent found that only 13 studies were included, largely from South Africa and others from Uganda, Zambia, and the Democratic Republic of Congo (DRC). The review findings suggest varying efficacy of SUD treatment modalities across the continent and a critical gap in longitudinal research from other African countries to inform scalable, evidence-based solutions for SUD treatment/management.
In Kenya, Kasisi
applied the Cox PH model to data from Mathari National Hospital to identify significant covariates for recovery: age, gender, employment status, and marital status. It was determined that gender (HR of 0.7316), job status (HR of 1.7629), marital status (HR of 0.4915), and age (HR of 1.2830) are significant predictors of recovery rates of individuals under treatment. Besides, married and employed individuals under treatment reported high survival rates, with average survival times of 19 and 18 months, respectively.
Additionally, the insights from other regional contexts reinforce the need for localized models. For example, Tlali et al.
| [21] | M. Tlali et al., “Diagnosis and treatment of opioid-related disorders in a South African private sector medical insurance scheme: A cohort study,” International Journal of Drug Policy, vol. 109, p. 103853, Nov. 2022,
https://doi.org/10.1016/j.drugpo.2022.103853 |
[21]
used Cox PH models in South Africa to analyze opioid-related disorders and treatment engagement in private healthcare, showing a rise in mortality risk among individuals with opioid-related disorders. These findings underscore the need to use survival analysis techniques, particularly the Cox PH model, to understand recovery from SUDs so that mortality risk from this condition can be reduced.
The existing literature on drug addiction recovery has primarily focused on relapse rates or qualitative aspects, with limited application of survival analysis in the Kenyan context. Kasisi
used the Cox PH model to identify predictors like age and gender. Still, they did not evaluate other potential predictors like education level, and did not compare recovery rates between alcohol and multiple-drug addiction. Their strength lies in identifying significant demographic covariates, but they exclude other potentially cognitive-significant predictors and comparisons across substance types, potentially limiting the tailoring of interventions.
Besides, the use of other models, such as logistic regression by Lu et al.
| [12] | W. Lu, T. Lopez-Castro, and T. Vu, “Population-based examination of substance use disorders and treatment use among US young adults in the National Survey on Drug Use and Health, 2011–2019,” Drug and Alcohol Dependence Reports, vol. 8, p. 100181, Sep. 2023,
https://doi.org/10.1016/j.dadr.2023.100181 |
[12]
to examine SUD prevalence and treatment, suggests the opportunity to model recovery from SUD using the Cox PH model, provided the data meet the proportional hazards assumption. Therefore, this study expands the prior Kenyan and other identified studies by incorporating other/different predictors as covariates and comparing alcohol versus multiple-drugs addiction recovery rates. Using the Cox PH model, this study estimated recovery rates and identified significant predictors, addressing the lack of localized, quantitative studies (as noted by
| [19] | F. Jaguga et al., “A systematic review of substance use and substance use disorder research in Kenya,” PLOS ONE, vol. 17, no. 6, p. e0269340, Jun. 2022,
https://doi.org/10.1371/journal.pone.0269340 |
| [20] | C. Biribawa et al., “Treatment outcomes for substance use disorders across the African continent: a systematic review,” BMC Psychology, vol. 13, no. 1, Jul. 2025,
https://doi.org/10.1186/s40359-025-02978-5 |
[19, 20])
to inform targeted interventions in high-burden areas of Kenya and similar regional settings. Particularly, this study aimed to construct a Cox PH model to estimate hazard rates for recovery in drug-addicted individuals in Kericho County and identify significant predictors of recovery from drug addiction using the model.
2. Materials and Methods
2.1. Data Collection, Preprocessing, and Analysis
Secondary data was obtained from Palm Tree House Wellness Center in Kericho County, which provides drug abuse and psychiatric treatment. The secondary ensured consistency in treatment records, reducing potential bias introduced by new data collection. The data collection involved obtaining the relevant information from the patient files kept and provided by the facility. The records for each patient admitted to the facility were kept in individual files. Data entry was performed to record all relevant details in an Excel spreadsheet. The follow-up period for data collection was 2021 to 2025.
Data was then cleaned by removing fields that do not provide details about the covariates for analysis. Missing values were handled using median imputation for continuous variables and category expansion for categorical variables to minimize information loss (there were a few missing entries, but no entry was missing the event or censoring). The missing categorical values for categorical variables were replaced with the “Unknown” category. For example, if an entry for marital status was missing, the marital status of that observation was indicated as “Unknown.”
Data analysis was conducted using the R statistical package. The Cox PH model was developed for specific covariates (age, period of addiction, education level, job status, marital status, and substance type). A 5% level of significance was used to assess the significance of the covariates in the Cox PH model, the overall model significance, and the proportional hazards assumption. This level of significance was adopted because it aligns with conventional statistical practice and balances the risks of Type I and Type II errors.
2.2. Research Design
This study employed a retrospective observational research design, analyzing existing data to model recovery from drug addiction. The Cox PH model assessed the effects of covariates on recovery rates. Recovery times were recorded in days, with recovery defined as discharge from the rehabilitation center. Purposive sampling of secondary data records was used, selecting all patient records that met the study inclusion criteria during the study period for analysis. The inclusion criteria required that each patient record have a clearly defined recovery time and event indicator. Individuals were included if they either recovered from addiction or were censored due to incomplete recovery or early exit from treatment. Records with missing survival time or outcome status were excluded.
A total of 186 eligible records of individuals undergoing treatment for drug addiction were obtained. Since this was a retrospective study, the sample size was determined by the availability of complete patient records rather than prospective calculation. The adequacy of the sample size was assessed using the events-per-variable (EPV) criterion recommended for Cox PH modeling. Particularly, for Cox proportional hazards models, a minimum of 10 events per covariate is recommended
.
Six covariates were used in this study, implying a minimum of 60 required events. The collected data comprised 159 events; therefore, the sample size was deemed sufficient to yield reliable and stable hazard ratio estimates. Specifically, the 10 events-per-variable rule provides a minimum threshold rather than an optimal sample size. Although six covariates require at least 60 events, this study used the full dataset to ensure greater statistical power and to produce more stable, reliable, and precise Cox PH model estimates.
2.3. Cox PH Model Specifications
The Cox PH model assumes proportional hazards, and the baseline hazard rate is not specified and is arbitrary for continuous time 𝑇, unlike in the parametric proportional hazards model, where the baseline hazard represents the specific distribution of the hazard rate
| [11] | Xian Liu, Survival analysis: models and applications. Chichester, West Sussex: Wiley, 2012. |
[11]
. The following equation gives the Cox PH model:
Where
are the regression coefficients,
are the covariates and
is the number of covariates being studied
| [2] | D. R. Cox, “Regression Models and Life-Tables,” Journal of the Royal Statistical Society. Series B (Methodological), vol. 34, no. 2, pp. 187–220, 1972, Available:
https://www.jstor.org/stable/2985181 |
[2]
. The model is the product of the baseline hazard function,
and the exponential expression.
The baseline hazard function is the hazard for the reference individual with covariate values of 0. The reference individuals in this study were alcohol-addicted, as the study sought to compare alcohol-addicted versus multiple-drug-addicted individuals adjusted for other covariates. It is assumed that the effects of are multiplicative, so the predicted for will fall in the range. The hazard ratios (HRs) of the covariates were generated by the exponentiation of the corresponding regression coefficients.
The model is called a proportional hazards model because the baseline hazard function does not depend on the explanatory variable, and the exponential function does not depend on t, satisfying the assumption that the hazard ratios (HRs) for two groups (e.g., alcohol-only vs. multiple-drug addiction) are constant over time.
Considering the desired event in this study (recovery from drug addiction), the hazard function provided the rate at which an individual attains recovery at a given time . Therefore, a high hazard rate corresponded to a fast recovery from addiction. Some of the covariates in this study (age and period of addiction) are continuous, which require continuous versions of the hazard and cumulative hazard functions. In this study, the were assumed to be time-independent to satisfy the assumption. Although some variables, such as age, would change over time under normal circumstances, they are appropriately treated as time-independent because they did not change significantly throughout this study.
2.4. Model Diagnostics
The proportional hazards assumption was assessed using Schoenfeld residuals for each covariate and a global test of proportionality. Schoenfeld residuals were named after David Schoenfeld, who, in 1982, showed how to test the proportional hazards assumption using them
. Since, under the proportional hazards assumption, the effect of a covariate on the hazard is constant over time, the Schoenfeld residuals should not have a systematic association with time. Therefore, the Schoenfeld residual test formally assesses this relationship by examining if the residuals are correlated with time. If the test results are non-significant, the covariate effects do not change over time, thereby supporting the proportional hazards assumption.
In addition, the Wald statistics test was used to assess the significance of covariates, which tests whether the estimated regression coefficients differ significantly from zero. Wald tests give a straightforward assessment of whether an individual estimated coefficient differs significantly from zero, allowing for immediate interpretation of associated hazard ratios, confidence intervals, and p-values.
3. Results
3.1. Cox PH Model
The Cox PH model in equation (
2) was obtained.
Table 1 shows the model coefficients, hazard ratios, and p-values, identifying two primary significant predictors of recovery:
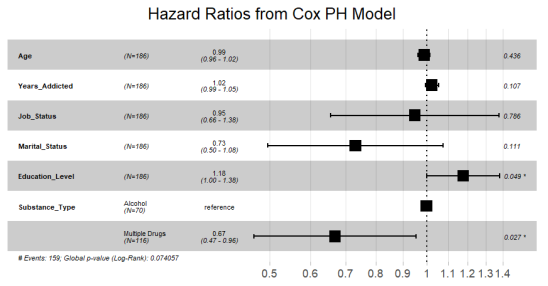
Education Level: Higher education level was associated with a higher hazard rate for recovery (HR = 1.18, p = 0.049). This suggests that for every unit increase in educational attainment, the hazard of recovery increases by 18%.
Substance Type (Multiple vs. Alcohol): Individuals using multiple substances (polysubstance use) had a significantly lower hazard rate for recovery compared to those using only alcohol (HR = 0.67, p = 0.027).
Table 1. Cox PH Model for Time to Recovery.
Covariate | Coef. | HR | SE | z | p-value | 95% CI for HR |
Age | -0.010 | 0.990 | 0.013 | -0.780 | 0.436 | (0.964, 1.016) |
Years Addicted | 0.024 | 1.024 | 0.015 | 1.611 | 0.107 | (0.995, 1.054) |
Job Status | -0.052 | 0.950 | 0.189 | -0.272 | 0.786 | (0.655, 1.377) |
Marital Status | -0.314 | 0.731 | 0.197 | -1.592 | 0.111 | (0.497, 1.075) |
Education Level | 0.162 | 1.176 | 0.082 | 1.966 | 0.049* | (1.001, 1.382) |
Substance Type | -0.404 | 0.668 | 0.183 | -2.207 | 0.027* | (0.467, 0.956) |
Equation (
2) is the resulting Cox PH model for time to recovery:
(2)
These results of the Cox PH model were graphically represented in
Figures 1 and 2.
Figure 1. Hazard Ratios from Cox PH Model.
The plot in
Figure 1 summarizes the results of the Cox PH model, showing the adjusted hazard ratios (HR) for each predictor variable in relation to the outcome (recovery from drug addiction), while controlling for all other variables in the model.
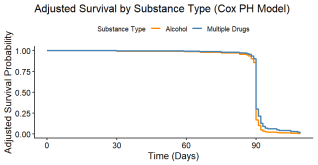
The adjusted survival curves (accounting for age, period of addiction, job status, marital status, and education level) show that individuals with multiple drug use experienced modestly higher survival probabilities (slower recovery rates) compared to alcohol-only users. This was particularly evident around the period of highest event incidence (approximately day 90), consistent with the significant protective hazard ratio (HR 0.67, 95% CI 0.47–0.96, p=0.027). Both groups exhibited very low long-term survival, with most events occurring in a narrow late window.
Figure 2. Adjusted Survival by Substance Type.
3.2. Assessing the Proportional Hazards Assumption
The Schoenfeld residuals for assessing the proportional hazards assumption of the model are shown in
Table 2.
Table 2. Test of Proportional Hazards Assumption using Schoenfeld Residuals.
Covariate | χ2 | df | p-value |
Age | 0.536 | 1 | 0.460 |
Years Addicted | 1.735 | 1 | 0.190 |
Job Status | 1.226 | 1 | 0.270 |
Marital Status | 0.015 | 1 | 0.900 |
Education Level | 1.323 | 1 | 0.250 |
Substance Type | 0.000 | 1 | 0.990 |
GLOBAL | 8.020 | 6 | 0.240 |
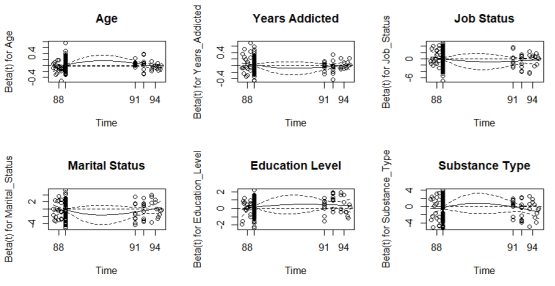
The Schoenfeld residual plots for the covariates are shown in
Figure 3.
Figure 3. Schoenfeld Residuals Plots.
4. Discussion
The results showed that higher education level was associated with a higher hazard rate for recovery (HR = 1.18, p = 0.049), suggesting that for every unit increase in educational attainment, the hazard of recovery increases by 18%. This finding implies that drug users with higher education levels may benefit, as far as recovery is concerned, from improved health literacy, better understanding of treatment goals, and greater adherence to counseling and rehabilitation programs/sessions. This supports theoretical frameworks such as health literacy and behavior change theories, as noted by Coughlin et al.
| [1] | S. S. Coughlin, M. Vernon, C. Hatzigeorgiou, and V. George, “Health literacy, Social Determinants of health, and Disease Prevention and Control,” Journal of Environment and Health Sciences, vol. 6, no. 1, 2020, Available:
https://pmc.ncbi.nlm.nih.gov/articles/PMC7889072/ |
[1]
, linking education to improved health-seeking behavior and treatment compliance.
On substance type, individuals using multiple substances (polysubstance use) had a significantly lower hazard rate for recovery compared to those using only alcohol (HR = 0.67, p = 0.027). This finding implies that polysubstance users have a 33% lower hazard of recovery at any given time compared to alcohol-only users. The slower recovery among the group addicted to multiple drugs may be attributed to higher dependency severity on them, increased likelihood of poly-substance use (which can lead to complex health issues and increased risks of overdose and addiction), and greater psychological and physiological withdrawal challenges. Previous addiction recovery studies like those by Ellis et al.
| [5] | J. D. Ellis, J. A. Rabinowitz, O. D. Ware, J. Wells, K. Dunn, and A. Huhn, “Patterns of polysubstance use and clinical comorbidity among persons seeking substance use treatment: An observational study,” Journal of Substance Use and Addiction Treatment, vol. 146, p. 208932, Jan. 2023,
https://doi.org/10.1016/j.josat.2022.208932 |
[5]
and Daigre et al.
| [3] | C. Daigre et al., “Treatment retention and abstinence of patients with substance use disorders according to addiction severity and psychiatry comorbidity: A six-month follow-up study in an outpatient unit,” Addictive Behaviors, vol. 117, p. 106832, Jun. 2021, https://doi.org/10.1016/j.addbeh.2021.106832 |
[3]
have reported similar findings, showing that recovery from addiction to multiple substances often requires longer and more intensive treatment compared to alcohol-only dependence. While it may seem intuitive that addiction to multiple drugs leads to slower recovery, the study statistically quantified this effect and demonstrated its significance using survival analysis. The Cox PH model shows that individuals addicted to multiple substances have a lower recovery hazard even after controlling for other factors, providing empirical evidence rather than relying on assumptions.
Age was not significantly associated with time to recovery (HR=0.99, p=0.436). The hazard ratio associated with this covariate indicates that an individual who is 1 year older experienced a 1% decrease in the recovery rate, although this effect was not statistically significant. Period of addiction was not significantly associated with recovery time (HR = 1.02, p = 0.107), even though longer duration was associated with a slight increase in recovery rate (i.e., a 1-year increase in the period of addiction was associated with a 2% increase in the hazard of recovery).
In addition, job status was not significantly associated with time to recovery (HR = 0.95, p = 0.786). Although employed drug users were associated with 5% decrease in recovery rate as compared to unemployed ones, this effect was not statistically significant. Similarly, marital status did not have a statistically significant effect on time to recovery (HR = 0.73, p = 0.111). Although the hazard ratio suggests that married/engaged individuals experience a 27% decrease in recovery rate compared to those who are not married (single, separated, divorced, widowed), this effect was not statistically significant (only directionally significant).
For model adequacy, the model demonstrated strong statistical adequacy, as shown in
Table 2, with the global proportional hazards assumption check yielding a p-value of 0.24, indicating no significant violation of the PH assumption. Additionally, the p-values for individual covariates were greater than 0.05, indicating no violation of the PH assumption. The Schoenfeld residual plots for covariates in
Figure 3 also show no evidence of violation of the proportional hazards assumption. Each plot displays the scaled Schoenfeld residuals over time, along with a smoothed curve and reference lines. The residuals are randomly scattered around zero, and the smoothed curves fluctuate around a horizontal line with no systematic upward or downward trend, indicating no variation of covariate effects over time.
The findings have direct implications for integrating evidence-based tailoring into Kenya’s national rehabilitation programs and NACADA-led policies. The 2025 National Policy for the Prevention, Management and Control of Alcohol, Drugs and Substance Abuse
| [22] | Ministry of Interior and National Administration, “National Policy for the Prevention, Management and Control of Alcohol, Drugs and Substance Abuse 2025,” 2025.
https://www.nacada.go.ke/node/1125 (accessed Apr. 02, 2026). |
[22]
prioritizes expanding access to quality, affordable treatment, rehabilitation, and aftercare services in every county. In the same way, NACADA’s Strategic Plan 2023–2027
emphasizes county-level rehabilitation facilities and data-driven programming to address the high burden of substance use disorders (SUDs). Therefore, in practice, the rehabilitation centers should incorporate education-stratified interventions. For individuals with low education levels, their rehabilitation programs could embed directed health literacy modules, simplified psycho-education sessions, and community-based learning tools within the residential or outpatient frameworks; this will strengthen the understanding of treatment goals, improve adherence, and accelerate recovery, directly supporting the policy’s objective of person-centered, holistic care. For individuals addicted to multiple drugs, treatment facilities should adopt differentiated care pathways containing extended residential stays, counseling that is more intensive, integrated management of co-occurring physical and mental health issues, and specialized withdrawal protocols.
For policy-making, NACADA and the Ministry of Health should integrate these predictors (education level and substance type) into updates to national standards and treatment protocols. This integration can involve developing guiding principles for substance-type stratification and education-informed care, directing the routine collection of these covariates in standardized data systems across facilities, and allocating resources preferentially to polysubstance programs. These steps would enhance recovery from drug addictions and reduce relapse, enhance the cost-effectiveness of the treatment, and contribute to the broader goal of reducing the economic burden of drug abuse while advancing the efforts on strengthening prevention and treatment of substance abuse.
Based on the findings of this study, future research should explore time-varying covariates to better assess changes in recovery risk or rates across different stages of treatment. In addition, conducting prospective cohort studies in the future would ensure the capture of additional psychosocial variables (e.g., level of family support and relapse history) and clinical variables (e.g., treatment intensity and duration).
5. Conclusions
This study used the Cox PH model to model the recovery from drug addiction among drug users under treatment in a rehabilitation center in Kericho County, Kenya, between 2021 and 2025. The findings showed that the significant predictors of recovery time were education level and substance type. The drug users addicted to multiple drugs had slower recovery than those addicted to alcohol only, while those with a higher education level experienced faster recovery than those with lower education levels. The factors that were found to have no significant association with recovery after adjustment were age, job status, marital status, and years of addiction.
The appropriateness of the Cox PH model for recovery time was confirmed by the proportional hazards assumption being satisfied. This study gives empirical evidence that substance-related and cognitive-social factors, rather than demographic factors alone, strongly influence recovery from drug addiction.
The study results are essential in offering recommendations towards the provision of treatment to drug users. For practice, the findings help rehabilitation centers understand factors that influence recovery duration and the groups of drug users that may require longer treatment, helping them improve treatment planning and patient monitoring. One recommendation is that these facilities should implement substance-specific treatment strategies, with more prolonged and intensive interventions for drug users addicted to multiple substances.
Secondly, treatment facilities should incorporate educational and health literacy components into treatment programs, especially for drug users with lower education levels; this will improve understanding, adherence, and engagement with treatment plans. Thirdly, clinicians need to prioritize early identification of individuals at risk of delayed recovery based on the substance type they are addicted to and tailor counseling intensity accordingly, for example, increasing the number of counseling sessions for them or having enhanced treatment approaches for them.
For policy, the findings of this study can help policymakers design targeted intervention programs for high-risk groups. Specifically, treatment programs could be structured differently for individuals with polysubstance addiction by incorporating more intensive therapy, longer rehabilitation periods, and specialized counseling services. Policymakers can also support the development of integrated treatment approaches that address both substance dependency and related psychological or social factors.
In addition, the authorities at the county and national levels should support standardized data collection systems in rehabilitation facilities. The systems, like those used in hospitals, should facilitate the systematic collection, processing, and analysis of information about drug users, which is crucial for evidence-based clinical research and for improving drug users’ outcomes.
Abbreviations
PH | Proportional Hazards |
HR | Hazard Ratio |
NACADA | National Agency for the Campaign Against Drug Abuse |
SUD | Substance Use Disorder |
UNODC | United Nations Office on Drugs and Crime |
Author Contributions
Victor Kiptoo Rotich: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Visualization, Writing – original draft
Benard Cheruiyot Tonui: Supervision
Joseph Kipyegon Cheruiyot: Supervision
Reuben Cheruiyot Lang’at: Supervision
Data Availability Statement
The data is available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
S. S. Coughlin, M. Vernon, C. Hatzigeorgiou, and V. George, “Health literacy, Social Determinants of health, and Disease Prevention and Control,” Journal of Environment and Health Sciences, vol. 6, no. 1, 2020, Available:
https://pmc.ncbi.nlm.nih.gov/articles/PMC7889072/
|
| [2] |
D. R. Cox, “Regression Models and Life-Tables,” Journal of the Royal Statistical Society. Series B (Methodological), vol. 34, no. 2, pp. 187–220, 1972, Available:
https://www.jstor.org/stable/2985181
|
| [3] |
C. Daigre et al., “Treatment retention and abstinence of patients with substance use disorders according to addiction severity and psychiatry comorbidity: A six-month follow-up study in an outpatient unit,” Addictive Behaviors, vol. 117, p. 106832, Jun. 2021,
https://doi.org/10.1016/j.addbeh.2021.106832
|
| [4] |
D. Das, H. Saikia, D. Bora, D. Bhattacharjee, and J. Das, “A survival analysis approach for identifying the risk factors in time to recovery of COVID-19 patients using Cox proportional hazard model,” Decision Analytics Journal, vol. 5, p. 100137, Dec. 2022,
https://doi.org/10.1016/j.dajour.2022.100137
|
| [5] |
J. D. Ellis, J. A. Rabinowitz, O. D. Ware, J. Wells, K. Dunn, and A. Huhn, “Patterns of polysubstance use and clinical comorbidity among persons seeking substance use treatment: An observational study,” Journal of Substance Use and Addiction Treatment, vol. 146, p. 208932, Jan. 2023,
https://doi.org/10.1016/j.josat.2022.208932
|
| [6] |
T. Iswardani, Z. L. Dewi, W. W. Mansoer, and I. Irwanto, “Meaning-Making among Drug Addicts during Drug Addiction Recovery from the Perspective of the Meaning-Making Model,” Psych, vol. 4, no. 3, pp. 589–604, Sep. 2022,
https://doi.org/10.3390/psych4030045
|
| [7] |
R. Kasisi, “Application of Cox Regression in Modeling Survival Rate of Drug Abuse,” American Journal of Theoretical and Applied Statistics, vol. 7, no. 1, p. 1, 2018,
https://doi.org/10.11648/j.ajtas.20180701.11
|
| [8] |
S. Kim and H. S. Suh, “A population-based study on the risk of prescription opioid abuse in patients with chronic opioid use and cost-effectiveness of prescription drug monitoring program using a patient simulation model in South Korea,” International Journal of Drug Policy, vol. 112, p. 103953, Feb. 2023,
https://doi.org/10.1016/j.drugpo.2023.103953
|
| [9] |
D. G. Kleinbaum and M. Klein, Survival Analysis. New York, NY: Springer New York, 2012.
https://doi.org/10.1007/978-1-4419-6646-9
|
| [10] |
W. Ling et al., “Recovery From Opioid Use Disorder (OUD) After Monthly Long-acting Buprenorphine Treatment,” Journal of Addiction Medicine, vol. 14, no. 5, Mar. 2020,
https://doi.org/10.1097/adm.0000000000000647
|
| [11] |
Xian Liu, Survival analysis: models and applications. Chichester, West Sussex: Wiley, 2012.
|
| [12] |
W. Lu, T. Lopez-Castro, and T. Vu, “Population-based examination of substance use disorders and treatment use among US young adults in the National Survey on Drug Use and Health, 2011–2019,” Drug and Alcohol Dependence Reports, vol. 8, p. 100181, Sep. 2023,
https://doi.org/10.1016/j.dadr.2023.100181
|
| [13] |
T. F. Martinelli, D. Roeg, L. Bellaert, van, and G. E. Nagelhout, “Understanding the Process of Drug Addiction Recovery Through First-Hand Experiences: A Qualitative Study in the Netherlands Using Lifeline Interviews,” Qualitative Health Research, vol. 33, no. 10, pp. 857–870, Jun. 2023,
https://doi.org/10.1177/10497323231174161
|
| [14] |
M. Moeeni, E. M. Razaghi, K. Ponnet, F. Torabi, S. A. Shafiee, and T. Pashaei, “Predictors of time to relapse in amphetamine-type substance users in the matrix treatment program in Iran: a Cox proportional hazard model application,” BMC Psychiatry, vol. 16, no. 1, Jul. 2016,
https://doi.org/10.1186/s12888-016-0973-8
|
| [15] |
NACADA, “National Survey on the Status of Drugs and Substance use in Kenya, Abridge Version,” 2022. Available:
https://nacada.go.ke/node/784
|
| [16] |
D. Schoenfeld, “Partial residuals for the proportional hazards regression model,” Biometrika, vol. 69, no. 1, pp. 239–241, 1982,
https://doi.org/10.1093/biomet/69.1.239
|
| [17] |
UNODC, “World Drug Report 2023,” United Nations: Office on Drugs and Crime, 2023.
https://www.unodc.org/unodc/en/data-and-analysis/world-drug-report-2023.html
|
| [18] |
D. Bochere and T. Mwendwa, “NACADA wants youth to shun drugs, substance use,” Kenya News Agency, Jul. 24, 2022.
https://www.kenyanews.go.ke/nacada-wants-youth-to-shun-drugs-substance-use/
(accessed Mar. 19, 2026).
|
| [19] |
F. Jaguga et al., “A systematic review of substance use and substance use disorder research in Kenya,” PLOS ONE, vol. 17, no. 6, p. e0269340, Jun. 2022,
https://doi.org/10.1371/journal.pone.0269340
|
| [20] |
C. Biribawa et al., “Treatment outcomes for substance use disorders across the African continent: a systematic review,” BMC Psychology, vol. 13, no. 1, Jul. 2025,
https://doi.org/10.1186/s40359-025-02978-5
|
| [21] |
M. Tlali et al., “Diagnosis and treatment of opioid-related disorders in a South African private sector medical insurance scheme: A cohort study,” International Journal of Drug Policy, vol. 109, p. 103853, Nov. 2022,
https://doi.org/10.1016/j.drugpo.2022.103853
|
| [22] |
Ministry of Interior and National Administration, “National Policy for the Prevention, Management and Control of Alcohol, Drugs and Substance Abuse 2025,” 2025.
https://www.nacada.go.ke/node/1125
(accessed Apr. 02, 2026).
|
| [23] |
NACADA, “National Authority for the Campaign Against Alcohol and Drug Abuse (NACADA),” Nacada.go.ke, 2023.
https://nacada.go.ke/index.php/node/912
(accessed Apr. 02, 2026).
|
Cite This Article
-
APA Style
Rotich, V. K., Tonui, B. C., Cheruiyot, J. K., Lang’at, R. C. (2026). Survival Analysis of Recovery from Drug Addiction Using the Cox Proportional Hazards Model. American Journal of Theoretical and Applied Statistics, 15(2), 72-80. https://doi.org/10.11648/j.ajtas.20261502.15
 Copy
|
Copy
|
 Download
Download
ACS Style
Rotich, V. K.; Tonui, B. C.; Cheruiyot, J. K.; Lang’at, R. C. Survival Analysis of Recovery from Drug Addiction Using the Cox Proportional Hazards Model. Am. J. Theor. Appl. Stat. 2026, 15(2), 72-80. doi: 10.11648/j.ajtas.20261502.15
Copy
|
Download
AMA Style
Rotich VK, Tonui BC, Cheruiyot JK, Lang’at RC. Survival Analysis of Recovery from Drug Addiction Using the Cox Proportional Hazards Model. Am J Theor Appl Stat. 2026;15(2):72-80. doi: 10.11648/j.ajtas.20261502.15
Copy
|
Download
-
@article{10.11648/j.ajtas.20261502.15,
author = {Victor Kiptoo Rotich and Benard Cheruiyot Tonui and Joseph Kipyegon Cheruiyot and Reuben Cheruiyot Lang’at},
title = {Survival Analysis of Recovery from Drug Addiction Using the Cox Proportional Hazards Model},
journal = {American Journal of Theoretical and Applied Statistics},
volume = {15},
number = {2},
pages = {72-80},
doi = {10.11648/j.ajtas.20261502.15},
url = {https://doi.org/10.11648/j.ajtas.20261502.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajtas.20261502.15},
abstract = {Drug addiction remains a critical public health challenge, particularly in developing countries like Kenya, where access to effective rehabilitation services is limited. Understanding the factors that influence recovery time is essential for improving treatment outcomes and informing evidence-based interventions. This study aimed to model recovery time among drug-addicted individuals using survival analysis techniques and to identify key determinants influencing the rate of recovery. This study focuses on applying the Cox PH model to estimate recovery hazard rates and identify significant predictors among individuals receiving treatment. A retrospective cohort design was employed using secondary data obtained from a rehabilitation facility in Kericho County, Kenya, covering the period 2021 to 2025. The key findings indicate that education level (HR 1.18, p=0.049) and Substance Type (Multiple Drugs vs. Alcohol, HR 0.67, p=0.027) are significant predictors of recovery from drug addiction. Specifically, higher education levels are associated with a higher hazard of recovery, likely due to enhanced health literacy. At the same time, individuals using multiple substances face a lower hazard of recovery compared to those using alcohol only, reflecting the clinical complexity of polysubstance use. The Cox PH model satisfied the proportional hazards assumption (Global p=0.24), confirming its adequacy for the data. These results highlight the importance of socio-demographic and substance-related factors in recovery from drug addiction. In practice, treatment facilities/rehabilitation centers should integrate health literacy enhancement programs specifically for individuals with lower education levels to improve treatment adherence and accelerate recovery. Besides, more intensive and prolonged interventions, such as enhanced counseling, specialized therapy, and closer monitoring, are recommended for polysubstance users to address their greater clinical needs. For policy, the study’s results underscore the need to develop substance-specific treatment guidelines, increase resource allocation for polysubstance addiction programs, and implement standardized drug-user data recording systems in rehabilitation facilities across Kenya. These strategies will improve recovery outcomes, optimize service delivery, and strengthen national efforts for reducing the burden of drug addiction.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Survival Analysis of Recovery from Drug Addiction Using the Cox Proportional Hazards Model
AU - Victor Kiptoo Rotich
AU - Benard Cheruiyot Tonui
AU - Joseph Kipyegon Cheruiyot
AU - Reuben Cheruiyot Lang’at
Y1 - 2026/04/21
PY - 2026
N1 - https://doi.org/10.11648/j.ajtas.20261502.15
DO - 10.11648/j.ajtas.20261502.15
T2 - American Journal of Theoretical and Applied Statistics
JF - American Journal of Theoretical and Applied Statistics
JO - American Journal of Theoretical and Applied Statistics
SP - 72
EP - 80
PB - Science Publishing Group
SN - 2326-9006
UR - https://doi.org/10.11648/j.ajtas.20261502.15
AB - Drug addiction remains a critical public health challenge, particularly in developing countries like Kenya, where access to effective rehabilitation services is limited. Understanding the factors that influence recovery time is essential for improving treatment outcomes and informing evidence-based interventions. This study aimed to model recovery time among drug-addicted individuals using survival analysis techniques and to identify key determinants influencing the rate of recovery. This study focuses on applying the Cox PH model to estimate recovery hazard rates and identify significant predictors among individuals receiving treatment. A retrospective cohort design was employed using secondary data obtained from a rehabilitation facility in Kericho County, Kenya, covering the period 2021 to 2025. The key findings indicate that education level (HR 1.18, p=0.049) and Substance Type (Multiple Drugs vs. Alcohol, HR 0.67, p=0.027) are significant predictors of recovery from drug addiction. Specifically, higher education levels are associated with a higher hazard of recovery, likely due to enhanced health literacy. At the same time, individuals using multiple substances face a lower hazard of recovery compared to those using alcohol only, reflecting the clinical complexity of polysubstance use. The Cox PH model satisfied the proportional hazards assumption (Global p=0.24), confirming its adequacy for the data. These results highlight the importance of socio-demographic and substance-related factors in recovery from drug addiction. In practice, treatment facilities/rehabilitation centers should integrate health literacy enhancement programs specifically for individuals with lower education levels to improve treatment adherence and accelerate recovery. Besides, more intensive and prolonged interventions, such as enhanced counseling, specialized therapy, and closer monitoring, are recommended for polysubstance users to address their greater clinical needs. For policy, the study’s results underscore the need to develop substance-specific treatment guidelines, increase resource allocation for polysubstance addiction programs, and implement standardized drug-user data recording systems in rehabilitation facilities across Kenya. These strategies will improve recovery outcomes, optimize service delivery, and strengthen national efforts for reducing the burden of drug addiction.
VL - 15
IS - 2
ER -
Copy
|
Download